Introduction of Education Systems for Clinical Engineers in Japan
Jun Yoshioka1,2,Keiko Fukuta2,Hiroki Igeta2,Takeshi Ifuku2,Tadayuki Kawasaki2
1.Department of Clinical Engineering,Yamagata University Hospital,Yamagata 990-9585,Japan;2.International Exchange Committee,Japan Association for Clinical Engineers,Japan
Abstract:Japanese clinical engineer (CE) is a signifcant and unique profession compared with other nations with its dual clinical and technology focus and national licensing. The CE system of licensing was established in May 1987 under the Clinical Engineers Act. CEs are required to complete 3 to 4 years in designated schools and pass a national examination. It is a professional medical position responsible for the operation and maintenance of life-support and non-life-support medical device systems under the direction of physicians. Currently approximately 70 educational institutes-including technical colleges and universities-provide diverse and wide-ranging curricula from engineering to various clinical disciplines to produce CEs. Since clinical practice training is mandatory as a part of institute work,an important approach for CEs is gained by working in hospitals. The comprehensive curricula and the licensing system in Japan together serve to keep the appropriate quantity and quality of CEs. The Japan Association for Clinical Engineers (JACE) was established in February 1990;one of its aims is to support improvement of CEs throughout their careers through various lectures,seminars,on-the-job trainings,workshops,and an annual member meeting. New CEs can now take advantage of video e-learning. For junior CEs,there are seminars for hyperbaric oxygen therapy,blood purification,heart-lung bypass,respiratory therapy,operating room,intensive care unit,arrhythmia and aphaeresis related devices,as well as healthcare technology management (HTM). Also,the institutes provide a leadership seminar alongside this clinical practice training. Besides the licensing process,a proper certifcation system for CEs is a critical element in the clinical feld. This enhances the ability of CEs to engage in more extensive duties and develop specialties,as well as to provide better healthcare. Associated societies provide certifcation with technology qualifcations in dialysis,extracorporeal circulation,respiratory therapy,clinical medical devices,hyperbaric oxygen therapy,and aphaeresis treatment. JACE also launched a unique certifcation system in 2010,with specializations in blood purifcation,arrhythmia,respiratory,and hyperbaric oxygen care. What is the difference between certification by the associated societies and that offered by JACE? Certifcation by the associated societies provides basic knowledge to pass specialty examinations. Certifcations by JACE promote deeper knowledge to enhance clinical decisionmaking and to encourage wider experience. JACE also continues to investigate other certifcations. In summary,Japan has introduced a national licensing system for keeping an intake of constant quality and quantity of CEs. Additionally,ongoing workshops and seminars stimulate in-depth knowledge and a higher level of medical care for patients. Together,a system of lifelong education for CEs has been built.
Keywords:Japanese clinical engineer;Japan Association for Clinical Engineers;national license;certifcation system
1 INTRODUCTION
It is important to ensure appropriate quality control of medical equipment support. For example,physicians and nurses throughout the world typically manage medical equipment in the hospital such as mechanical ventilators and anesthesia machines[1-3]. In the past in Japan,physicians and nurses performed daily operation of mechanical ventilators[4];and faulty ventilators were repaired by the distributor. However,since the late 1990s,clinical engineers (CEs),who have a certificate of completion and have met and completed established course requirements,now perform the daily operation and maintenance of medical equipment in hospitals. We introduce the national licensing system for keeping a constant quality and quantity of CEs,as well as ongoing workshops and seminars that increase further in-depth knowledge for CEs as they provide care and support.
2 WHAT ARE JAPANEASE CES
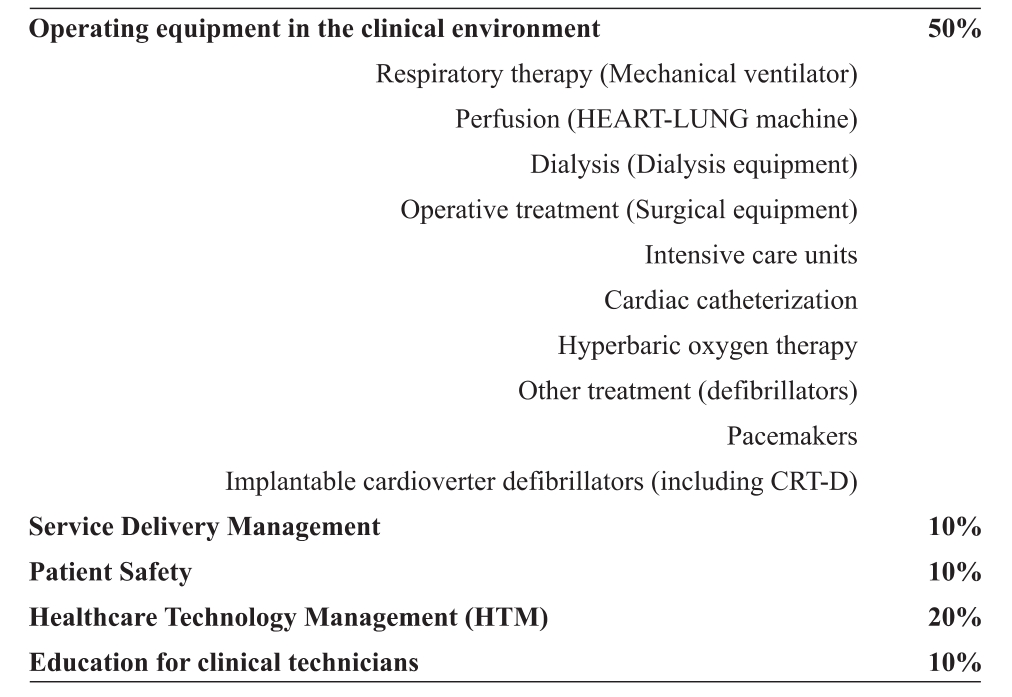
The CE role in Japan is a paramedical profession that is unique. CEs are medical technologists who work in the clinical field in hospitals and operate and maintain various medical equipment,such as mechanical ventilators,hemodialysis,heart-lung machines,and other medical devices. The demand for CEs is high,and the number of CEs has increased steadily since the specialty was introduced in May 1987. As of April 2015,there are about 35,000 CEs working in Japan and the CE membership number has been growing by about 2,000 every year. CEs are required to complete 3 to 4 years of study in designated schools and pass a national examination. CE is a professional medical position responsible for the operation and maintenance of life-support and non-life-support systems under the direction of physicians. The CE familiar with medical equipment operation can train physicians and nurses how to best use the equipment,as operator mistakes account for many malfunctions. Proper education on correct usage is a critical element in the clinical field. Clinical engineers actively work in a broad variety of clinical areas such as the operating room,dialysis,cardiac catheterization,hyperbaric oxygenation,ICU,HCU,NICU,emergency room and the general hospital ward,as well as conducting service delivery management,patient safety,HTM and educational initiatives (Table 1).
Table 1 Business operations:Japan clinical engineers
3 DESIGNATED SCHOOLS
Approximately seventy educational institutes-including technical colleges and universities-provide diverse and wide-ranging curricula from engineering to various clinical disciplines to produce CEs. Since clinical practice training is mandatory as part of institute work,an important approach for CEs is gained by working in a hospital. Robust curricula and the licensing system in Japan together serve to keep the appropriate quantity and quality of CEs.
4 JAPAN ASSOCIATION FOR CLINICAL ENGI-NEERS
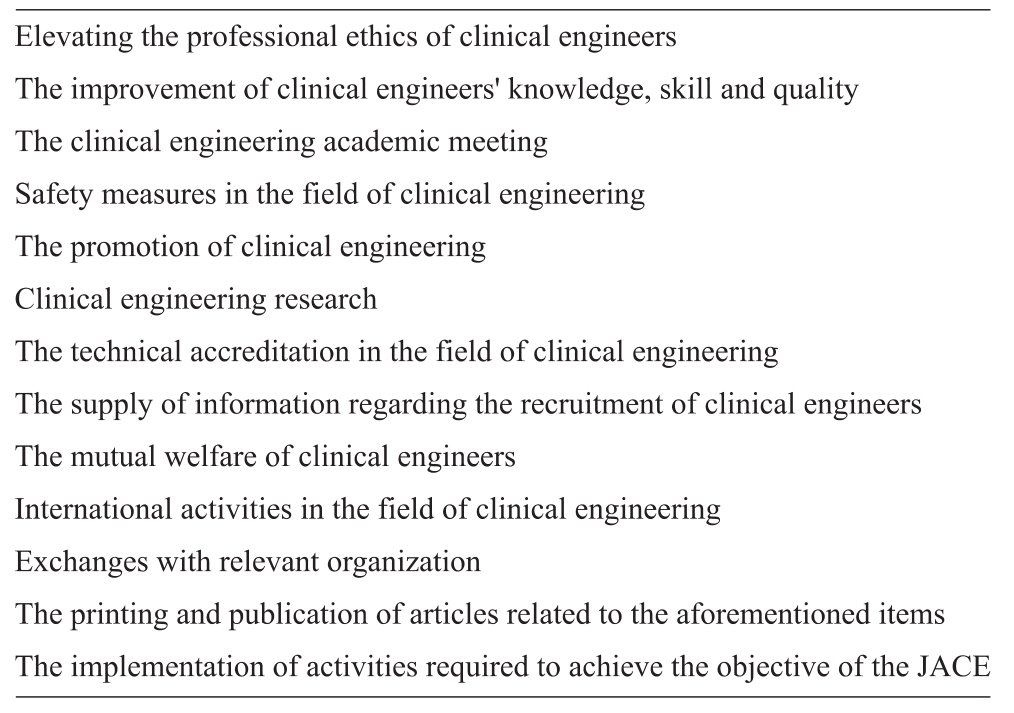
The Japan Association for Clinical Engineers (JACE) was established in February 1990. In a bid to accomplish its social mission,expand the duties and raise the status of CEs,the Ministry of Health,Labor,and Welfare (MHLW) approved JACE as Public-interest Corporation on March 14,2002. Twenty years have already passed since JACE was first established. During this time,the importance of medical equipment in modern medical care has been greatly enhanced and consequently,the social responsibility of CEs for handling such equipment has increased and there are currently 15,000 JACE members working in Japan. Table 2 shows JACE’s range of activities to achieve its objectives. One of its aims is to support improvement of CEs throughout their careers through various lectures,seminars,on-the-job trainings,workshops,and an annual member meeting. New CEs can now take advantage of video e-learning. There is a leadership seminar for institutes providing clinical practice training. Also,for junior CEs,there are seminars for hyperbaric oxygen therapy,blood purifcation,heart-lung bypass,respiratory therapy,operating room,intensive care unit,arrhythmia and aphaeresis related devices,as well as HTM.
5 CERTIFICATION SYSTEM
A proper certification system for CEs is a critical elementin the clinical feld. This enhances the ability of CEs to engage in more extensive duties and develop specialties,as well as to provide better healthcare. For certification by associated societies,there are technology qualifications in dialysis,extracorporeal circulation,respiratory therapy,clinical medical devices,hyperbaric oxygen therapy,and aphaeresis treatment. JACE also launched a unique certification system in 2010,with specializations in blood purifcation,arrhythmia,respiratory,and hyperbaric oxygen care. What is the difference between certification by the associated societies and by the JACE? Certifcation by the associated societies provides basic knowledge to pass specialty examinations. Certifications by JACE promotes deeper knowledge to enhance academic ability and stimulate wider experience. JACE also continues to investigate other certifcations.
Table 2 Constitution of the Japan Association for Clinical Engineers







































































































































































































6 ANNUAL MEETING
JACE holds an annual meeting,in addition to regional meetings such as in Tohoku,Kanto,and Kyushu. The JACE 2015 congress had about 5,000 participants,utilizing hotels and international conference centers for about 500 oral presentations,120 posters,40 exhibitors,and several lectures,symposia,workshops,and luncheon seminars. The number of participants and presentations has been increasing each year.
7 KIDS SEMINAR
JACE wants to encourage children to consider clinical engineering. Thus JACE is hosting awareness building activities,built around various medical equipment such as incubators,defibrillators,infusion pumps,syringe pumps,external pacemakers,mechanical ventilators,dialysis machines,heart lung machines and other medical equipment. In all,there have been over 300 participants. Children gain useful experiences by operating the equipment,and their smiles make us happy. The public relations campaign in promoting the children’s seminar helped to gain publicity for CEs.
8 INTERNATIONAL EXCHANGE COMMITTEE
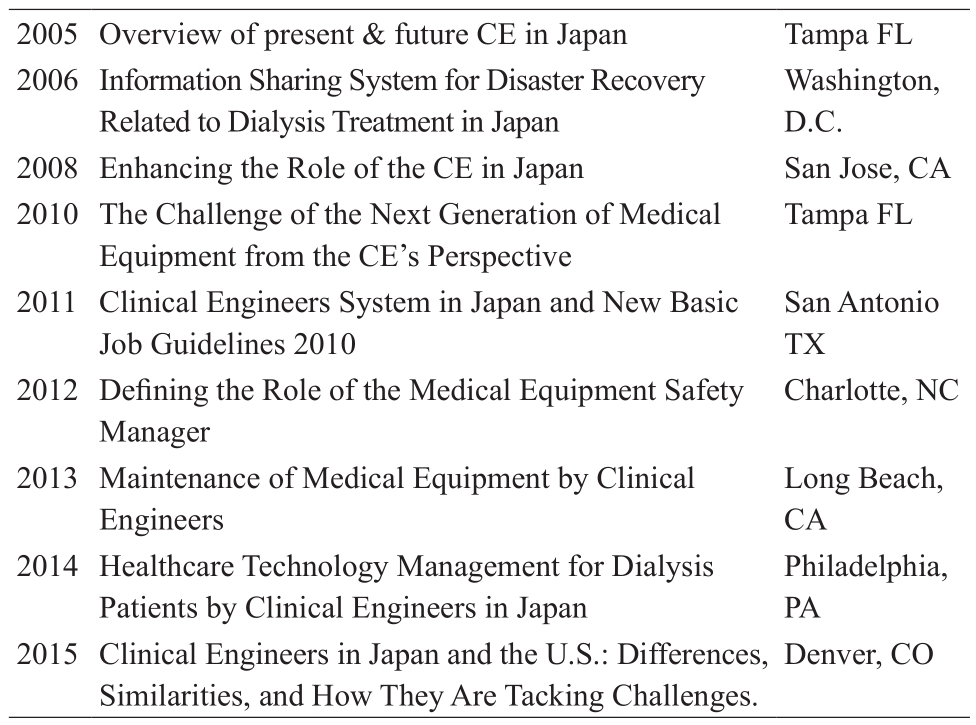
JACE has the International Exchange Committee (IEC) has three main aims. First,closer communication with other industrialized nations and information collection through positive participation in international programs. Next,technological cooperation in the areas of CE and blood purification,including transfer of CE systems and exchange with China. And last,dissemination of a CE mindset and development of an international orientation through participating in Japan Overseas Cooperation Volunteers Program as well as the Senior Volunteers Program of Japan International Cooperation Agency. Additionally,IEC has made presentations at educational sessions presented by Association for the Advancement of Medical Instrumentation Annual Conference and Expo from 2005 to present and returns a lot of useful information to JACE's members (Table 3). IEC supports CEs who want to spread their wings around the world,and is determined to further safety management and HTM.
Table 3 Presentations given at the Association for the Advancement of Medical Instrumentation
How do you know if medical equipment is reliable,accurate,and safe? Safety management as part of HTM is an important safety approach. In earlier years,equipment was simple and rugged,and did not break down easily[5]. Operator error accounted for most sudden malfunctions[6,7]. However,in present day,technology development has led to significant improvements in high performance medical equipment[8-11]. Modern critical care medical equipment has numerous CPU boards and sensors,and more failure points[12]. Thus,increased equipment support and safety focus as part of HTM by clinical engineering is necessary. CEs in Japan are increasingly adding these activities.
9 PROSPECTS FOR THE FUTURE
Clinical engineering is an essential profession for the safeoperation of medical equipment. CE in Japan has decreased medical equipment failure that exposed patients to potentially harmful risks. JACE members are learning some established HTM best practices through American CEs,viathe American College of Clinical Engineering (ACCE) programs. Therefore it is important to continue to introduce ACCE's advanced CE education system in Japan. Whereas Japanese CEs operate and maintain high technology devices,American CEs primarily focus on life cycle management activities-increasingly including devices integrated with electronic medical records and other health IT systems-as well as oversee clinical technicians who maintain equipment. Both professions are very important in HTM in the world.
10 CONCLUSION
CEs,who are medical technologists working in hospitals,are unique to Japan. The involvement of CEs in operating and maintaining medical equipment has proven to be important to hospitals,ensuring prompt service and increased safety. CE has become an essential profession.
11 ACKNOWLEDGMENTS
We recognize members of ACCE,USA for their helpful and constructive comments on this article. The Japan Association for Clinical Engineers also appreciates ACCE for their faithful service to their country during the tragic 2011 Tsunami.
[REFERENCES]
[1]Chapkowski S,Pucilo NP,Cane RD,et al.Impact on ventilatorcheck time of an in-circuit computerized respiratory monitoring system[J].Respir Care,1984,29:144-146.
[2]Association of Anaesthetists of Great Britain and Ireland (AAGBI),Hartle A,Anderson E.Checking anaesthetic equipment 2012:association of anaesthetists of Great Britain and Ireland[J].Anaesthesia,2012,67:660-668.
[3]Bourgain JL,Baguenard P,Puizillout JM,et al.The breakdown of anesthesia equipment survey[J].Ann Fr Anesth Reanim,1999,18:303-308.
[4]Chapkowski S,Pucilo NP,Cane RD,et al.Impact on ventilatorcheck time of an in-circuit computerized respiratory monitoring system[J].Respir Care,1984,29:144-146.
[5]Richard JCM,Kacmarek RM.ICU mechanical ventilators,technological advances vs. user friendliness:the right picture is worth a thousand numbers[J].Intensive Care Med,2009,35:1662-1663.
[6]Blanch PB.Mechanical ventilator malfunctions:a descriptive and comparative study of 6 common ventilator brands[J].Respir Care,1999,44:1183-1192.
[7]Vignaux L,Tassaux D,Jolliet P.Evaluation of the userfriendliness of seven new generation intensive care ventilators[J].Intensive Care Med,2009,35:1687-1691.
[8]Richard JC,Carlucci A,Breton L,et al.Bench testing of pressure support ventilation with three different generations of ventilators[J].Intensive Care Med,2002,28:1049-1057.
[9]Tassaux D,Michotte JB,Gainnier M,et al.Expiratory trigger setting in pressure support ventilation:from mathematical model to bedside[J].Crit Care Med,2004,32:1844-1850.
[10]Thille AW,Lyazidi A,Richard JC,et al.A bench study of intensive-care-unit ventilators:new versus old and turbinebased versus compressed gas-based ventilators[J].Intensive Care Med,2009,35:1368-1376.
[11]Marchese AD,Chipman D,de la Oliva P,et al.Adult ICU ventilators to provide neonatal ventilation:a lung simulator study[J].Intensive Care Med,2009,35:631-638.
[12]Chatburn RL.Computer control of mechanical ventilation[J].Respir Care,2004,49:507-517.
专栏——公共卫生与人体健康信息监测-Part Ⅱ
编者按:随着经济的飞速发展,掠夺性资源开发造成的空气污染、土壤污染、水污染、沙漠化和生态失衡等问题,已直接威胁着人类自身的健康。对公共环境卫生和自身健康信息的监测是预防重大疾病、保障和促进人体健康的重要手段。在本专栏Part II系列文章中,主要介绍基于微流控芯片的环境卫生检验分析系统及装置、用于检测动脉内皮功能的电阻抗和热分析方法、基于智能移动终端的低成本心音采集系统、体位对桡动脉脉搏波影响的量化分析等,为公共环境卫生和人体健康信息监测提供一定的参考。
[CLC number]R197.39 [Document code]A
doi:10.3969/j.issn.1674-1633.2016.09.001
[Article ID]1674-1633(2016)09-0001-04
Correspondence to:Jun Yoshioka,Department of Clinical Engineering,Yamagata University Hospital,2-2-2 Iidanishi,Yamagata 990-9585,Japan.